Groundhog Day – COVID & “The Science”
Tyler Durden
Mon, 11/30/2020 – 16:20
Authored by Raul Ilargi Meijer via The Automatic Earth,
When politicians across the globe tell you they listen to “the science” when defining their COVID measures, they don’t really, they are lying. What they listen to is a shred of science as formulated by their local virologists and epidemiologists, which is inevitably questioned by other scientists.
If this were not the case, the entire world would now be taking the same measures, and there would not be any discussions in the scientific community. Still, when measures are imposed in various countries, they are imposed as some kind of law. Lockdowns are popular among failed and failing politicians, because they see it as a failsafe measure (there’s nothing more extreme). But that is only because they have never moved beyond the “COVID is the only problem we have” mindframe.
Still, even then, it would be wise to recognize these measures as arbitrary. That’s why they differ from one place to another; they make it up as they go along, guided by their limited understanding of the issue. What US Supreme Court Justice Neil Gorsuch opined on New York Governor Andrew Cuomo’s decree on closing churches, as the court struck down the decree, is a fine example of why they are arbitrary:

Things tend to be better defined when courts of law rule on them. That’s what courts are for. Which is why we should pay attention when a Portuguese court states that PCR tests are 97% unreliable. We don’t pay attention, because our media ignore that ruling. And we continue to use the PCR test on a massive scale, even if its own inventor says it shouldn’t be used for this purpose. And so says the box that it comes in. “The science”? No, it’s not.
And for all those countries that close their stores and schools, this from Canada should perhaps, no, definitely, open eyes:
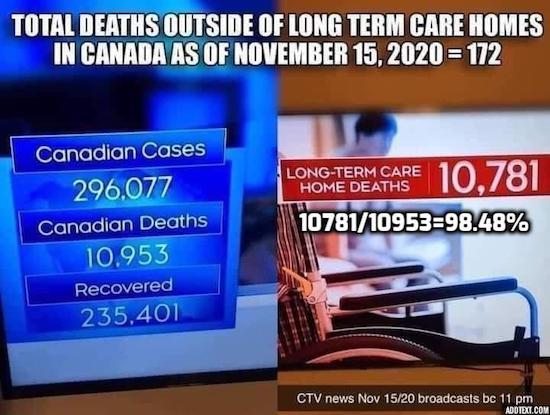
If only 1.5% of COVID deaths happen outside of long term care homes, the “science” doesn’t say close your schools and stores and make everyone wear a mask 24 hours a day, the science says pump massive amounts of resources into those care homes in order to stop the misery there. Closing stores will not do that. It will have other, very negative, effects though, while you’re not taking care of the care homes.
This is from Peter Andrews, a geneticist and science journalist: Landmark Legal Ruling Finds That Covid PCR Tests Are Not Fit For Purpose
Four German holidaymakers who were illegally quarantined in Portugal after one was judged to be positive for Covid-19 have won their case, in a verdict that condemns the widely-used PCR test as being up to 97% unreliable. Earlier this month, Portuguese judges upheld a decision from a lower court that found the forced quarantine of four holidaymakers to be unlawful. The case centred on the reliability (or lack thereof) of Covid-19 PCR tests. The verdict, delivered on November 11, followed an appeal against a writ of habeas corpus filed by four Germans against the Azores Regional Health Authority. This body had been appealing a ruling from a lower court which had found in favour of the tourists, who claimed that they were illegally confined to a hotel without their consent.
The tourists were ordered to stay in the hotel over the summer after one of them tested positive for coronavirus in a PCR test – the other three were labelled close contacts and therefore made to quarantine as well. The deliberation of the Lisbon Appeal Court is comprehensive and fascinating. It ruled that the Azores Regional Health Authority had violated both Portuguese and international law by confining the Germans to the hotel. The judges also said that only a doctor can “diagnose” someone with a disease, and were critical of the fact that they were apparently never assessed by one. They were also scathing about the reliability of the PCR (polymerase chain reaction) test, the most commonly used check for Covid.
The conclusion of their 34-page ruling included the following: “In view of current scientific evidence, this test shows itself to be unable to determine beyond reasonable doubt that such positivity corresponds, in fact, to the infection of a person by the SARS-CoV-2 virus.” In the eyes of this court, then, a positive test does not correspond to a Covid case. The two most important reasons for this, said the judges, are that, “the test’s reliability depends on the number of cycles used’’ and that “the test’s reliability depends on the viral load present.’’ In other words, there are simply too many unknowns surrounding PCR testing.
This is not the first challenge to the credibility of PCR tests. Many people will be aware that their results have a lot to do with the number of amplifications that are performed, or the ‘cycle threshold.’ This number in most American and European labs is 35–40 cycles, but experts have claimed that even 35 cycles is far too many, and that a more reasonable protocol would call for 25–30 cycles. (Each cycle exponentially increases the amount of viral DNA in the sample). [..] The Portuguese judges cited a study conducted by “some of the leading European and world specialists,” which was published by Oxford Academic at the end of September. It showed that if someone tested positive for Covid at a cycle threshold of 35 or higher, the chances of that person actually being infected is less than three percent, and that “the probability of… receiving a false positive is 97% or higher.”
Then there are the vaccines that everyone’s so hyped up about. Gilbert Berdine, MD, writing for the Mises Institute, has some questions about the Pfizer and Moderna mRNA vaccines (anything to do with why Twitter suspended the institute’s account)?
What exactly is a “case” of COVID? It can’t be a positive PCR test, not if those are only 3% reliable. So “the science” must be doing something wrong, and with them just about any government on the planet.
And yes, Pfizer and Moderna have dollar signs in their eyes. There are many questions about the AstraZeneca/Oxford vaccine, and I can’t help thinking they are linked to the fact that it’s not-for-profit. Likewise, the complete silence about Russia’s Sputnik V vaccine is also curious. We want to solve the problem only if our own scientists and the Big Pharma they work for can do it?
What The COVID Vaccine Hype Fails To Mention
Both trials have a treatment group that received the vaccine and a control group that did not. All the trial subjects were covid negative prior to the start of the trial. The analysis for both trials was performed when a target number of “cases” were reached. “Cases” were defined by positive polymerase chain reaction (PCR) testing. There was no information about the cycle number for the PCR tests. There was no information about whether the “cases” had symptoms or not. There was no information about hospitalizations or deaths. The Pfizer study had 43,538 participants and was analyzed after 164 cases. So, roughly 150 out 21,750 participants (less than 0.7%) became PCR positive in the control group and about one-tenth that number in the vaccine group became PCR positive.
The Moderna trial had 30,000 participants. There were 95 “cases” in the 15,000 control participants (about 0.6%) and 5 “cases” in the 15,000 vaccine participants (about one-twentieth of 0.6%). The “efficacy” figures quoted in these announcements are odds ratios. There is no evidence, yet, that the vaccine prevented any hospitalizations or any deaths. The Moderna announcement claimed that eleven cases in the control group were “severe” disease, but “severe” was not defined. If there were any hospitalizations or deaths in either group, the public has not been told.
When the risks of an event are small, odds ratios can be misleading about absolute risk. A more meaningful measure of efficacy would be the number to vaccinate to prevent one hospitalization or one death. Those numbers are not available. An estimate of the number to treat from the Moderna trial to prevent a single “case” would be fifteen thousand vaccinations to prevent ninety “cases” or 167 vaccinations per “case” prevented which does not sound nearly as good as 94.5% effective.
The publicists working for pharmaceutical companies are very smart people. If there were a reduction in mortality from these vaccines, that information would be in the first paragraph of the announcement.
There is no information about how long any protective benefit from the vaccine would persist. Antibody response following covid-19 appears to be short lived. Based on what we know, the covid vaccine may require two shots every three to six months to be protective. The more shots required, the greater the risk of side effects from sensitization to the vaccine. There is no information about safety. None. Government agencies like the Centers for Disease Control (CDC) appear to have two completely different standards for attributing deaths to covid-19 and attributing side effects to covid vaccines.
If these vaccines are approved, as they likely will be, the first group to be vaccinated will be the beta testers. I am employed by a university-based medical center that is a referral center for the West Texas region. My colleagues include resident physicians and faculty physicians who work with covid patients on a daily basis. I have asked a number of my colleagues whether they will be first in line for the new vaccine. I have yet to hear any of my colleagues respond affirmatively.
The reasons for hesitancy are that the uncertainties about safety exceed what they perceive to be a small benefit. In other words, my colleagues would prefer to take their chances with covid rather than beta test the vaccine. Many of my colleagues want to see the safety data after a year of use before getting vaccinated; these colleagues are concerned about possible autoimmune side effects that may not appear for months after vaccination.
Next, we get a look, through the American Institute for Economic Research, at a report that Johns Hopkins University somewhat mysteriously pulled from its website: New Study Highlights Alleged Accounting Error Regarding Covid Deaths
It is already well established that Covid-19 is a disease that is most dangerous to those over the age of 65 and who have preexisting conditions. In the United States, there has been an observed 2.1% mortality rate, with elderly individuals making up over half that number. Young and healthy people are not by any significant capacity threatened by Covid-19. One of the most important factors when it comes to Covid-19 is preventing excess death. According to the CDC, “Estimates of excess deaths can provide information about the burden of mortality potentially related to the COVID-19 pandemic, including deaths that are directly or indirectly attributed to COVID-19. Excess deaths are typically defined as the difference between the observed numbers of deaths in specific time periods and expected numbers of deaths in the same time periods.”
Essentially, there is an average number of deaths every year due to a variety of causes that for the most part have remained constant through the years. This includes morbidities such as heart disease, which has long been the leading cause of death, and cancer, which has long plagued our existence. For Covid-19 to be a serious cause of alarm, it would need to significantly increase the number of average deaths. However, according to the study, “These data analyses suggest that in contrast to most people’s assumptions, the number of deaths by COVID-19 is not alarming. In fact, it has relatively no effect on deaths in the United States.” Total deaths in the United States show no significant change and even mirror past trends of seasonal illness.
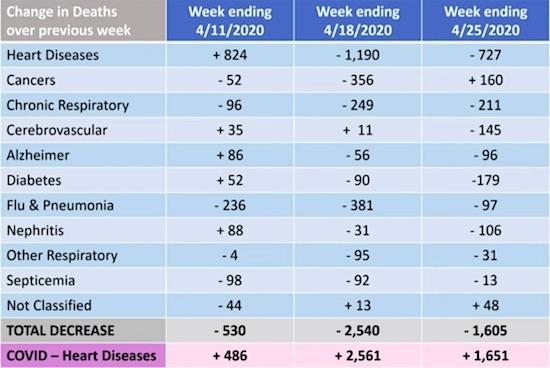
[..] What is even more interesting if not more alarming is that the spike in recorded Covid-19 deaths seen in 2020 has coincided with a proportional decrease in death from other diseases. Yanni Gu writes “This suggests, according to Briand, that the COVID-19 death toll is misleading. Briand believes that deaths due to heart diseases, respiratory diseases, influenza and pneumonia may instead be recategorized as being due to COVID-19.” Deaths have remained relatively constant, yet reported deaths due to deadly conditions such as heart disease have fallen while reported Covid deaths have risen. This suggests that the current Covid death count is in some capacity relabeled deaths due to other ailments. According to the graph, reported Covid deaths even overtook heart disease as the main cause of death at one point, which should raise suspicion.
And when you see the Clinical Infectious Diseases journal report that some 53 million American may already have been infected, you must ask what the use is of all the COVID measures at this point in time. If this is true in the US, chances are it is true in virtually any other location.
Looks like everybody has it and only people in care homes die from it, and on top of that many of those people didn’t actually die from COVID but from some other affliction. And for that we are closing down our entire societies, force massive amounts of businesses into bankruptcy, force millions upon millions into unemployment. All while relying on a test method that is 97% unreliable.
Total COVID19 Cases In US May Be Eight Times Higher Than Reported
The actual number of Covid-19 infections in the U.S. could be about eight times as much as the total reported cases, a model created by scientists at the Centers for Disease Control and Prevention (CDC) has estimated. The model published in the journal Clinical Infectious Diseases suggests that nearly 53 million people in the U.S. had been infected with Covid-19 by the end of September. The estimate is around eight times higher than the 7.1 million confirmed cases that had been reported back then. The model tries to account for the fact that most cases of Covid-19 are mild and therefore go unreported. The scientists, however, warned that by the end of September, 84% of the U.S. population had not been infected and was still at risk of catching the disease.
If the trend of unreported cases still holds true as of Thursday, the U.S. — which has 12.5 million confirmed cases — could be approaching 100 million total infections across the country. In October, the World Health Organisation had said that nearly 10% of the world population or nearly 760 million people may have already been infected with Covid-19, despite the fact that only 35 million confirmed cases had been recorded as of that time.
“When you count anything, you can’t count it perfectly,” Mike Ryan, the executive director of the WHO’s health emergencies program, had said back then adding, “But I can assure you that the current numbers are likely an underestimate of the true toll of Covid.” Scientists have also suggested that deaths due to the pandemic have also been severely undercounted, with the CDC stating that the U.S. had recorded nearly 300,000 excess deaths during the pandemic as of October 3. This number was nearly 100,000 deaths more than what had been officially recorded by the states.
What we need is actual science. Not “a science” or “some science”, but undisputed science. Einstein’s E=MC2 is science, that’s the level we need. Not disputable pseudo-science. Yes, there’s panic among politicians and scientists alike, yes, there is Long-COVID, yes there are people with multiple organ failure, but you will still have to do risk-assessment, you must look at how many people are involved.
And if you’re talking 0.01% of people, you need to wonder if it’s worthwhile to close down your entire society in a Great Reset kind of fashion. Likewise, forcing everyone to wear facemasks outside is something that must be evaluated as per risk factors. What is the risk of infecting anyone while just passing them in the street? It’s never zero, but no risk is ever zero. And if it’s 0.001%, does that justify turning your streets into a zombified society that puts everyone on edge?
“The science” needs to evolve, and it doesn’t appear to have done that. We’re back to square one all the time. COVID equals Groundhog Day. “Well, that didn’t help, so let’s do more of the same”. By now, the science, to remain believable, should have developed, moved on. It hasn’t. The hope for vaccines has taken on desperate levels, and the reliance on Big Pharma doesn’t help. Nor does the outright rejection of Russian, Chinese, Cuban vaccines. All nations with excellent medical resources, but ignored for political reasons. This is not the time to play politics. It’s a time for science to step up to the plate.

Are things much worse in countries that leave their stores open? Are they in places that don’t make people wear facemasks 24/7? The “science” should answer those questions by now. What else are they doing? But it’s not happening. COVID vs “The Science”: 1-0.
* * *